Article Review: A cost effectiveness study of PSMA PET CT for the detection of clinically significant prostate cancer
Objectives
- Evaluated the cost-effectiveness and quality of life impact of incorporating Prostate-Specific Membrane Antigen (PSMA) Positron Emission Tomography/Computed Tomography (PET/CT) into the current diagnostic algorithm for prostate cancer, which includes Prostate-Specific Antigen (PSA) testing and multiparametric Magnetic Resonance Imaging (mpMRI).
- Compared a standard of care MRI-driven diagnostic pathway to a strategy incorporating PSMA-PET/CT to potentially avoid unnecessary biopsies.
- Found that adding PSMA-PET/CT to MRI in patients with equivocal MRI findings (PI-RADS 3) is borderline cost-effective, while in men with negative MRI (PI-RADS 1-2) it is not.
Methodology
- A life-time decision model was used to compare the two diagnostic strategies.
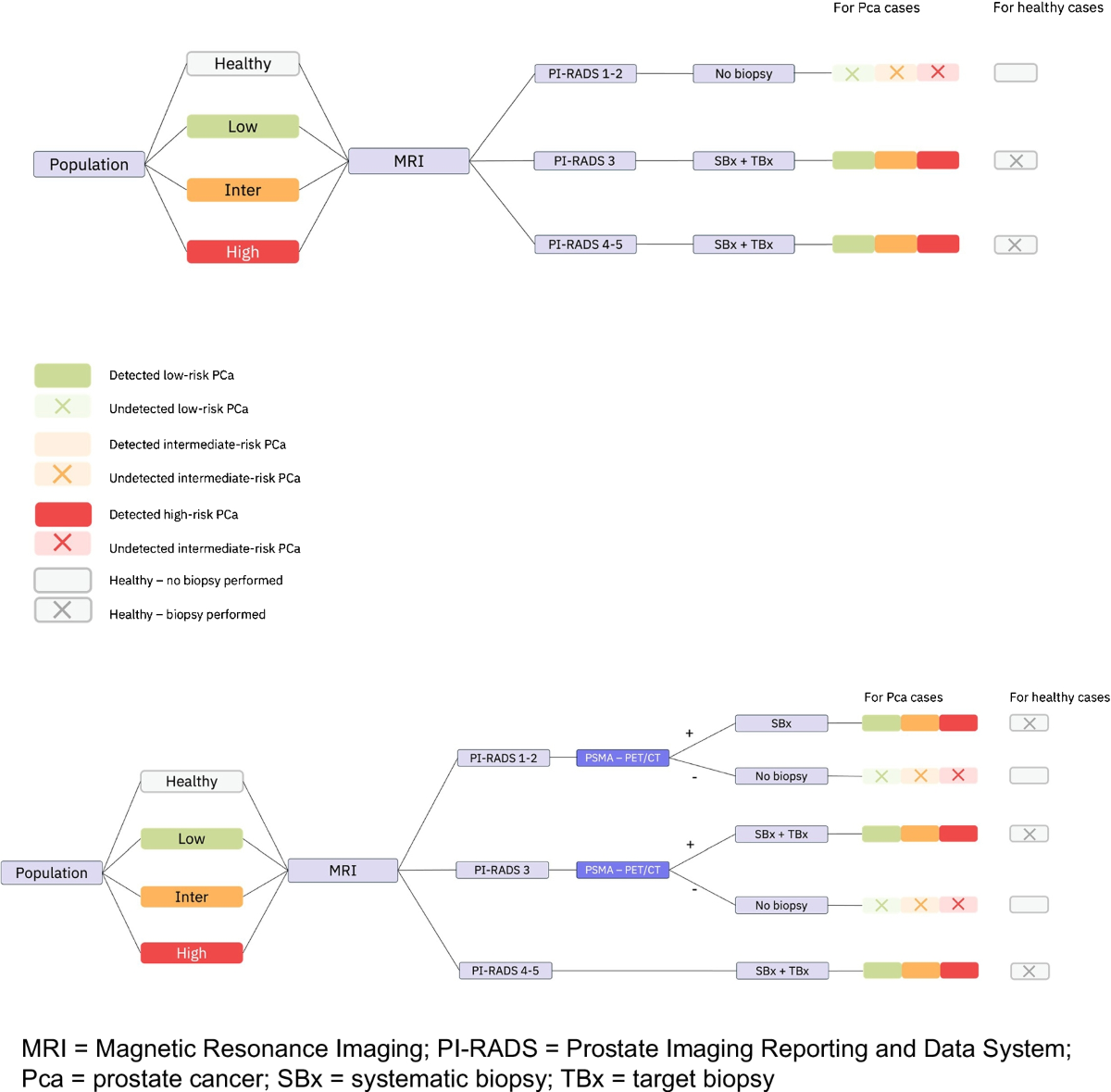
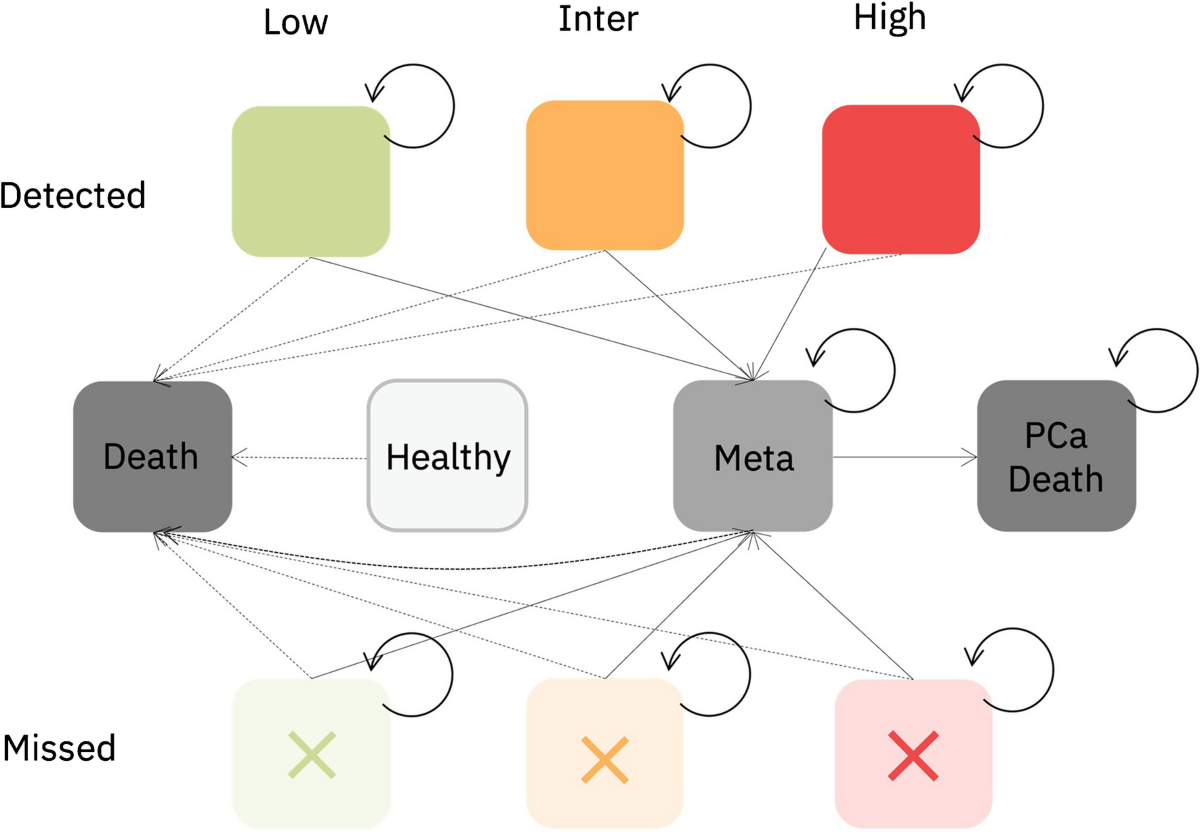
- The model combined a decision tree and a state transition model.
- Individual patients were simulated with a disease status and age.
- The decision tree represented the diagnostic and initial treatment pathway.
- The health state transition model represented patient follow-up and assessed the consequences of the diagnostic and treatment pathway outcomes.
- Long-term quality-adjusted life years (QALY) and healthcare costs were calculated for each approach.
- Model inputs included disease prevalence, treatment distributions, side effects, costs, quality of life values, progression rates, and mortality.
Results
- In PI-RADS 3 lesions, PSMA-PET/CT improved per-patient QALY by 0.002 and was borderline cost-effective, with an increased cost of €170-€186 per patient and an incremental cost-effectiveness ratio (ICER) of €56,700-€93,212 per QALY.
- In PI-RADS 1-2, PSMA-PET/CT led to a per-patient QALY decrease of 0.001 points, a cost increase of €416-€429 per patient, and was thus not cost-effective.
- In PI-RADS 3, PSMA-PET/CT could have prevented biopsies in 107 or 121 patients (out of 1000), but 10 or 14 low-risk prostate cancers would have remained undetected.
- In PI-RADS 1-2, 58 or 78 additional biopsies would have been performed, resulting in the diagnosis of 13 or 44 additional low-risk prostate cancers, 14 or 19 intermediate-risk, and 0 or 6 high-risk prostate cancers.
Discussions
- The study is limited by the relatively small sample sizes used for the PSMA-PET/CT outcomes, although different input models were utilized. Larger, phase 3 data is needed to confirm these findings.
- The study used Dutch healthcare costs, which may not be generalizable to other countries. Cost-effectiveness outcomes may vary depending on local intervention costs.
- The model assumes a PSMA-PET/CT cost of €1129, which is at the lower end of the price range. Strategies to further reduce costs are needed to expand PSMA-PET/CT use in earlier settings.
- The study used different tracers ([18F]PSMA-1007 vs. [68Ga]Ga-PSMA-11) in the initial study and the external PRIMARY1 trial, which could lead to different scan results and affect the generalizability of the findings.
1 views