Article Review: Diagnostic accuracy in NSCLC lymph node staging with Total Body and conventional PET CT
Objectives
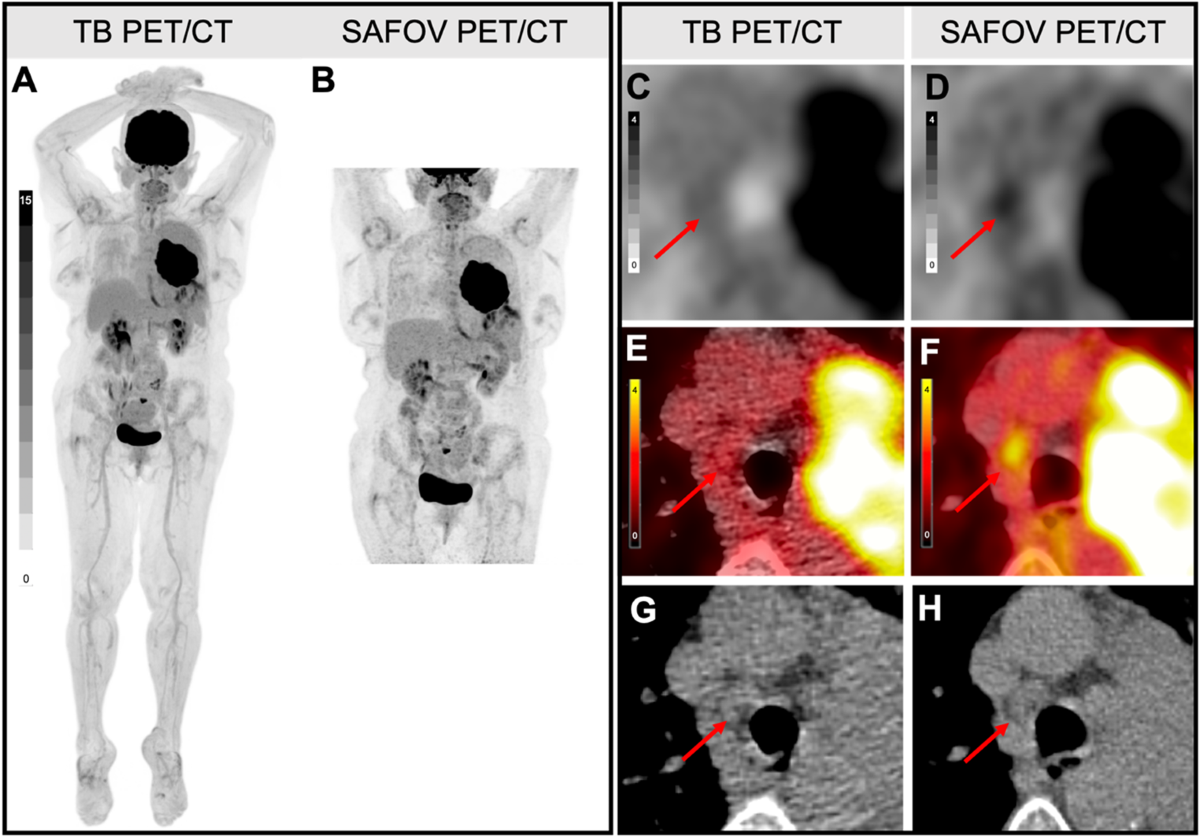
- This study prospectively compared the diagnostic accuracy of Total-Body (TB) PET/CT and conventional short-axial field-of-view (SAFOV) PET/CT for N-staging in non-small cell lung cancer (NSCLC) patients.
- TB PET/CT showed slightly higher sensitivity and positive predictive value (PPV) compared to SAFOV PET/CT, although not statistically significant.
- TB PET/CT had a lower rate of incorrect N-staging and lower semi-quantitative thresholds (Tumor-to-background ratio (TBR), Metabolic Tumor Volume (MTV), Total Lesion Glycolysis (TLG)) for detecting positive mediastinal lymph nodes.
Methodology
- A prospective, single-center, cross-over, head-to-head comparative study design was used.
- 48 NSCLC patients underwent [18F]FDG TB and SAFOV PET/CT on the same day.
- 700 lymph node levels from 28 patients were correlated with a composite reference standard (histopathology, imaging after treatment).
- Lymph nodes were characterized semi-quantitatively (SUVmax, TBR, MTV, TLG).
- TB PET images were reconstructed with TOF enabled OSEM, 4 iterations, 20 subsets.
- SAFOV PET images were reconstructed with TOF enabled OSEM, 2 iterations, 21 subsets.
Results
- TB PET/CT sensitivity: 86.0% (CI: 77.0–95.0%), specificity: 98.3% (CI: 97.3–99.3%), PPV: 81.7% (CI: 71.9–91.5%), NPV: 98.6% (CI: 97.9–99.6%).
- SAFOV PET/CT sensitivity: 77.2% (CI: 66.3–88.1%), specificity: 97.4% (CI: 96.1–98.6%), PPV: 72.1% (CI: 60.9–83.4%), NPV: 98.0% (CI: 96.9–99.1%).
- Incorrect N-staging: 6/28 (21.4%) for SAFOV, 1/28 (3.5%) for TB PET/CT.
- SUVmax threshold: 3.0 for both scanners.
- TB PET/CT thresholds: TBR 1.2, MTV 0.5 ml, TLG 1.0 ml.
- SAFOV PET/CT thresholds: TBR 1.7, MTV 1.0 ml, TLG 3.0 ml.
Discussions
- The study is limited by a small sample size (n=28 with composite reference standard), which may affect the statistical power and generalizability of the findings.
- Histopathological correlation was not available for all lymph nodes, relying on a composite reference standard, which may introduce bias.
- The imbalance between the two study arms (due to lost or incomplete follow-up) could impact the results.
- The study could benefit from a more detailed analysis of the discordant cases, including specific characteristics of the lymph nodes that led to misclassification by either TB or SAFOV PET/CT.
Reference: Diagnostic accuracy in NSCLC lymph node staging with Total Body and conventional PET CT